
Why old medicines and specific nutrition could be the key to recovery!
Living with Inflammatory Bowel Disease (IBD), like Crohn’s disease or ulcerative colitis, can feel like an endless battle for just a moment of relief. Even with the latest therapies, many patients still face the frustration of recurring flare-ups and a diminished quality of life. But there’s hope on the horizon! Medical science is on the brink of a major transformation. Instead of focusing solely on new, expensive medications, we’re now exploring "repurposing": a smart approach that involves using existing, safe drugs in conjunction with tailored nutrition. This shift means we’re moving away from just managing symptoms and towards truly healing the intestinal barrier and reprogramming the immune system.
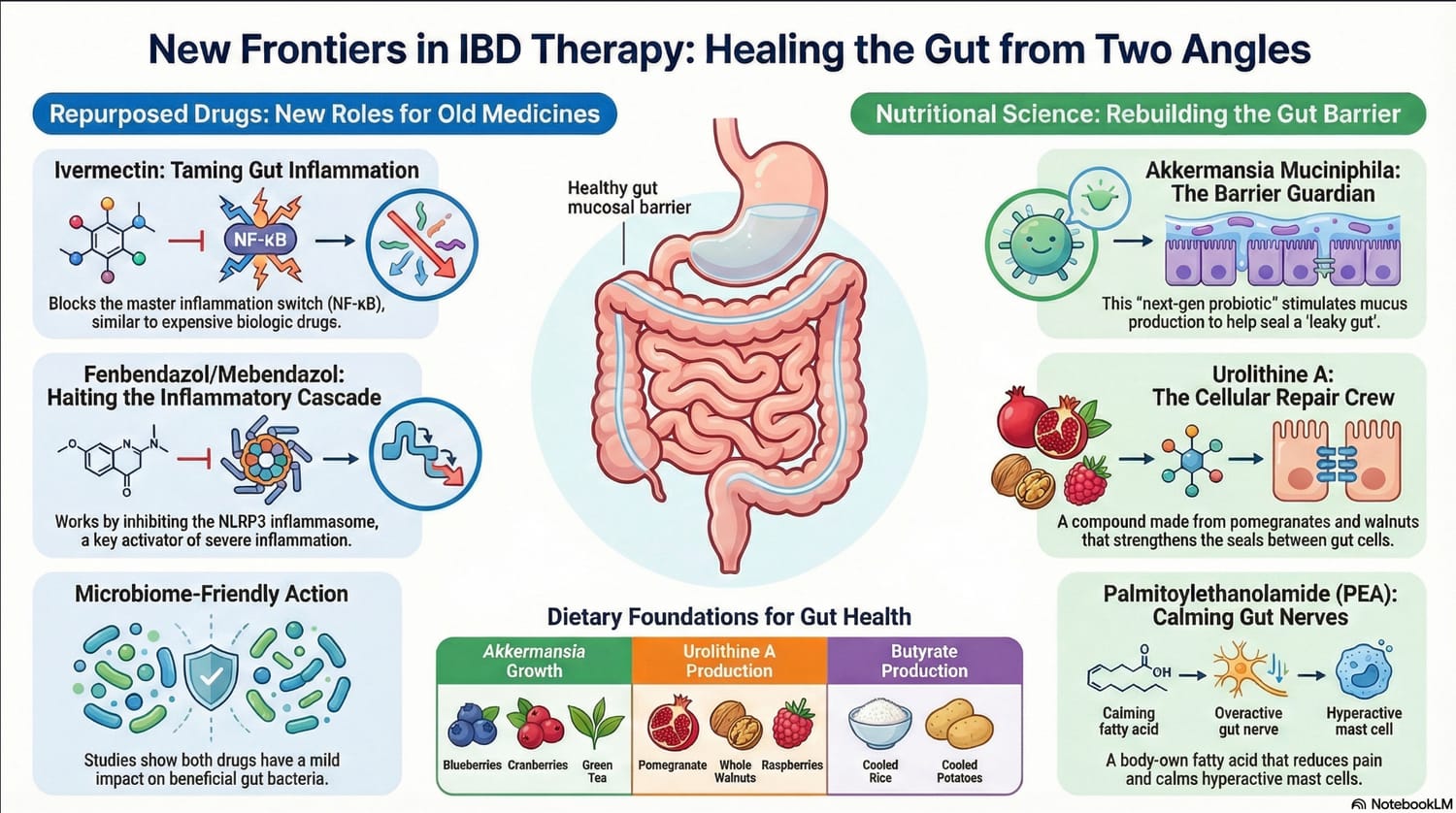
Ivermectin: More Than an Antiparasitic Agent
While Ivermectin is known worldwide for its effectiveness against parasites, recent clinical research reveals a much deeper layer. The drug serves as a powerful immune modulator capable of "taming" the inflammatory storm within the gut.
Ivermectin intervenes directly in the NF-κB pathway, the body’s central "master switch" for inflammation. By blocking this pathway, the production of harmful inflammatory proteins, such as TNF-α, is drastically reduced.
"By inhibiting the NF-κB pathway, Ivermectin targets the same biological markers as the costly biologicals that currently represent the gold standard in gastroenterology care."
Specialists in functional medicine examine specific receptors. Ivermectin acts as a positive allosteric modulator of the P2X4 receptor, which is essential for maintaining intestinal wall integrity and preventing "leaky gut." Furthermore, we observe a striking synergy with agents such as Baclofen via the GABAB receptors, which further enhances its anti-inflammatory potency.
From a scientific perspective, the human equivalent dose (HED) required for this effect is approximately 0.16 mg/kg. This is encouraging, as it is almost exactly the standard dosage that has been used safely for decades.
Fenbendazole and Mebendazole
Another group of medications gaining a second life in IBD care is the benzimidazoles. Agents such as Mebendazole and Fenbendazole (Panacur) have proven to be potent inhibitors of the NLRP3 inflammasome, a protein complex responsible for the most destructive inflammatory responses in intestinal tissue.
Fenbendazole warrants special attention due to its impact on B-cell maturation and the inhibition of the mTOR pathway. Although it sometimes causes a slight decrease in beneficial Lactobacillus in animal models, it is generally mild on the microbiome. Notably, a 2024 pilot study showed that Mebendazole resulted in a 20% higher remission rate in colitis patients when added as an adjuvant therapy.
A crucial pharmacological advantage of these agents is their poor systemic absorption. They remain largely within the gut, where they act directly on the sites of inflammation without causing severe systemic side effects.
Note on the Hygiene Hypothesis: While these agents are effective in adults, research by Vestergaard (2022) warns that early exposure (before the age of 5) may disrupt the maturation of the immune system. This underscores the critical importance of timing in therapy.
Akkermansia muciniphila: The 'Next-Gen' Guardian Angel
Effective gut restoration depends entirely on the presence of Akkermansia muciniphila. This bacterium is unique because it feeds on the mucus layer (mucin) of the intestinal wall. While this may seem destructive, this "mucus-eating" actually forces the gut to constantly renew its barrier and strengthen the tight junctions (the connections between intestinal cells).
The Biological Bridge
There is a fascinating biological bridge between medication and biology: through the modulation of the P2X4 receptor, Ivermectin helps stabilize microbial homeostasis, creating an ideal climate in which Akkermansia can flourish.
Precision Nutrition: Urolithin A and Mitophagy
A breakthrough in functional gastroenterology is the discovery of Urolithin A. This metabolite is produced by our gut flora from ellagitannins, which are found in pomegranates and walnuts.
Urolithin A activates mitophagy: the process by which cells clear out their defective energy factories (mitochondria). This is essential for "sealing" the intestinal wall.
The Microbial Nuance
It is important to realize that not everyone is capable of producing Urolithin A; this depends on the presence of specific gut bacteria. Therefore, "prebiotic priming" through the right foods and targeted supplementation is crucial.
Foods for Recovery:
Blueberries and Cranberries: Stimulate the growth of Akkermansia by a factor of 10 to 100.
Pomegranates and Walnuts: Provide the necessary raw materials for Urolithin A production.
Green Tea (EGCG): Acts as a powerful prebiotic for protective bacterial strains.
The Synergetic Protocol: A Daily Menu for the Gut
True healing occurs when we allow medication and nutrition to work in tandem. This protocol focuses on nourishing Akkermansia and inhibiting the same inflammatory pathways targeted by the previously mentioned medications.
Breakfast: The Polyphenol Bowl Chia pudding or oatmeal (soluble fibers) with a generous serving of blueberries and crushed walnuts. Pair this with green tea that has steeped for at least 5 minutes to ensure maximum EGCG release.
Lunch: The Barrier Salad Baby spinach with steamed salmon and pomegranate seeds. Use a generous amount of extra virgin olive oil; the Oleocanthal present in the oil works synergistically with Ivermectin by also inhibiting the NF-κB pathway.
Dinner: The Anti-Inflammatory Stir-fry Broccoli and bok choy prepared with fresh turmeric, ginger, and a pinch of black pepper (to maximize curcumin absorption).
Crucial Specialist Tip: The "Cook and Cool" Method
By allowing starchy foods such as rice or sweet potatoes to cool completely after cooking, resistant starch is formed. This is the primary fuel for Faecalibacterium prausnitzii, the most important producer of butyrate in our intestines and a crucial player in suppressing inflammation.
Noël
Sources & References
1. Preclinical Models & Anti-inflammatory Mechanisms
Research into the GABA$_B$ receptor, acetic acid-induced colitis, and NF-κB pathways is primarily based on a key 2022 study:
Aryannejad, A., et al. (2022). "Anti-inflammatory Effects of Ivermectin in the Treatment of Acetic Acid-Induced Colitis in Rats: Involvement of GABA$_B$ Receptors." Published in: International Immunopharmacology.
Key Findings: This study identified the synergistic effect between Ivermectin and Baclofen. It documented a decrease in TNF-$\alpha$, COX-2, iNOS, and MPO activity, specifically linking these effects to the downregulation of the p-NF-κB p65 pathway.
Zhang, X., et al. (2009). "Avermectin exerts anti-inflammatory effects by downregulating the nuclear transcription factor kappa-B and mitogen-activated protein kinase activation pathway." Published in: Fundamental & Clinical Pharmacology.
Key Findings: This foundational paper established that Ivermectin/avermectins inhibit LPS-induced inflammatory cytokine production by blocking NF-κB and MAPK (p38 and JNK) signaling.
He, J., et al. (2023). "P2X4 receptor modulates gut inflammation and favours microbial homeostasis in colitis." Published in: Clinical and Translational Medicine.
Key Findings: Using mouse models, this study demonstrated that Ivermectin acts as a positive allosteric modulator of the P2X4 receptor, alleviating DSS-induced colitis and stabilizing gut microbiota.
2. Gut Microbiome & Microbial Stability
Data regarding the Triple-SHIME system and the protective role of fibers originate from a 2023 publication:
Schoeman, A., et al. (2023). "Impact of Ivermectin on the Gut Microbial Ecosystem." Published in: International Journal of Molecular Sciences (MDPI).
Key Findings: Utilizing the Simulator of the Human Intestinal Microbial Ecosystem (SHIME), the study confirmed that Ivermectin caused only minor, temporary changes in healthy microbiomes. It showed that soluble fibers protected against drug-induced shifts and predicted an increase in short-chain fatty acid (SCFA) production.
3. Clinical Observations & Parasitic Co-infection
The clinical scenario involving Strongyloides stercoralis and the persistence of autoimmune inflammation is a recognized observation in gastroenterological literature:
Case Series/Report: e.g., Gut (BMJ Journal), "P101 Case series: Strongyloides stercoralis an important mimic of inflammatory bowel disease" (2023).
Context: These reports highlight that while Ivermectin effectively clears the parasite, the "mimicry" of IBD symptoms often requires standard IBD therapies (corticosteroids/biologicals) because the autoimmune process continues after the larvae are eradicated.
4. Safety & P-glycoprotein Transport
Edwards, G. (2003). "Ivermectin: Does P-glycoprotein play a role in neurotoxicity?" Published in: Filaria Journal.
Context: This pharmacological review discusses how Ivermectin is typically excluded from the brain by P-glycoprotein (P-gp) at the blood-brain barrier. High doses or P-gp inhibitors can lead to neurological toxicity.
Research on Benzimidazoles (Fenbendazole & Mebendazole)
Eskandari-Asgharzadeh, M., et al. (2022). "Mebendazole, an anti-helminth drug, suppresses inflammation, oxidative stress, and injury in a mouse model of ulcerative colitis." Published in: Scientific Reports.
Finding: Mebendazole (MBZ) significantly reduced colitis severity by lowering oxidative stress and suppressing inflammatory gene expression (IL-6 and TNF-$\alpha$).
Eskandari, M., et al. (2024). "Mebendazole as an Adjunct Therapy with Mesalamine to Increase Efficacy and Maintenance Therapy for Ulcerative Colitis Patients: A Pilot Study." (ClinicalTrials.gov: NCT06335160).
Finding: In a pilot study, adding 300–1000 mg/day of Mebendazole to standard care resulted in a faster decrease in Mayo scores and a 20% higher remission rate.
Vestergaard, T., et al. (2022). "Early-Life Mebendazole Exposure Increases the Risk of Adult-Onset Ulcerative Colitis." Published in: American Journal of Gastroenterology.
Finding: A large-scale Danish study found that children exposed to Mebendazole before age 5 had a higher risk of developing ulcerative colitis later in life, supporting the "hygiene hypothesis."
Medical Disclaimer
Please read this carefully.
Educational Purposes Only: The information on this website/blog is intended solely for educational and informational purposes. It is not intended as a substitute for professional medical advice, diagnosis, or treatment.
Not Medical Advice: I am not a physician or medical professional. Always consult a qualified doctor or healthcare provider before making changes to your diet, supplement routine, or medication use, especially if you have a pre-existing medical condition.
Assumption of Risk: Use of the information provided on this site is entirely at your own risk. The author is not liable for any side effects, complications, or negative consequences arising from the application of the discussed information or protocols.
No Guarantees: While we strive for accuracy, scientific insights evolve rapidly. We offer no guarantee that the information provided is complete, accurate, or up-to-date.
Off-Label Use: Some substances discussed may be used in a context that differs from officially approved indications (off-label). This is done for informational purposes only and does not constitute a recommendation.
In the event of a medical emergency, immediately contact a physician or call your local emergency services (e.g., 911 or 112).
Created by © Noël